
My appointment with my optometrist back in October led to a referral to see a specialist in Comox on November 12th. This appointment applied some interesting technology to my eye problem, and finally provided some resolution (ha ha).
In July, my optometrist used a device called a fundus camera to examine the retina in my right eye, as I was having some odd vision problems in that eye. The fundus is the inside, back surface of the eye. I’d had retinal photographs done before, so she could compare the current state of my retina to photos from years past. Retinal photography is, from a Geek’s perspective, kind of interesting, as you can actually see what the back of your eye looks like. According to UBC’s Department of Ophthalmology & Visual Sciences:
Color Fundus Retinal Photography uses a fundus camera to record color images of the condition of the interior surface of the eye, in order to document the presence of disorders and monitor their change over time.
A fundus camera or retinal camera is a specialized low power microscope with an attached camera designed to photograph the interior surface of the eye, including the retina, retinal vasculature, optic disc, macula, and posterior pole (i.e. the fundus).
Wikipedia gives a good example of what a normal fundus photograph should look like.
 |
 |
Normal fundus photographs of the right eye (left image) and left eye (right image), seen from front so that left in each image is to the person’s right. Each fundus has no sign of disease or pathology. The gaze is into the camera, so in each picture the macula is in the center of the image, and the optic disk is located towards the nose. Both optic disks have some pigmentation at the perimeter of the lateral side, which is considered normal (non-pathological). The orange appearance of the normal fundus is due to complexes of vitamin A as 11-cis-retinaldehyde with opsin proteins in the retina (i.e., rhodopsin). The left image (right eye) shows lighter areas close to larger vessels, which is regarded as a normal finding in younger people.
From my July retinal photographs, the optometrist thought the problem might be an “epiretinal membrane”; however, she wanted me to come in for another photograph in October to observe if there were any more changes.
Again, Wikipedia comes to the rescue and provides a pretty good description of what an “epiretinal membrane” is:
Epiretinal membrane or macular pucker is a disease of the eye in response to changes in the vitreous humor or more rarely, diabetes. Sometimes, as a result of immune system response to protect the retina, cells converge in the macular area as the vitreous ages and pulls away in posterior vitreous detachment (PVD). PVD can create minor damage to the retina, stimulating exudate, inflammation, and leucocyte response. These cells can form a transparent layer gradually and, like all scar tissue, tighten to create tension on the retina which may bulge and pucker, or even cause swelling or macular edema. Often this results in distortions of vision that are clearly visible as bowing and blurring when looking at lines on chart paper.
Interestingly, even though I’d never heard of epiretinal membranes (ERMs) before, they are relatively common. Most ERMs occur in individuals older than 50 years, and the likelihood of developing an ERM increases as age increases. Depending on the population being studied, the prevalence of ERMs varies from approximately 2% to 29%. Both sexes are equally affected. Most ERMs are asymptomatic. ERMs are a common complication associated with high myopia (which I have). There also appears to be a link between ERMs and immune system responses. At the time when I developed my eye problem, I was suffering a serious bout of “hayfever” triggered by alder pollen, with associated runny eyes and nose.
My retinal photograph in October was concerning enough that my optometrist referred me to the specialist in Comox. As I found out later, she was concerned that I might be developing something called a “macular hole”. The macula is part of the retina at the back of the eye. It is only about 5 mm across; however, it is responsible for our central vision, most of our colour vision and the fine detail of what we see. The macula has a very high concentration of photoreceptor cells – the cells that detect light. A macular hole is a small break in the macula. So, clearly a hole in the macula could have serious implications for a person’s vision.

So off I went to Comox in November. The ophthalmologist used a technique called optical coherence tomography (OCT), which essentially creates a cross sectional profile of the retina using a low energy red laser-like light. According to UBC’s Department of Ophthalmology & Visual Sciences:
Optical Coherence Tomography is a noninvasive imaging technology used to obtain high resolution cross-sectional images of the retina. The layers within the retina can be differentiated and retinal thickness can be measured to aid in the early detection and diagnosis of retinal diseases and conditions.
OCT testing has become a standard of care for the assessment and treatment of most retinal conditions. OCT uses rays of light to measure retinal thickness. No radiation or X-rays are used in this test, an OCT scan does not hurt and it is not uncomfortable.


Tomography is the creation of cross-sectional images using any kind of penetrating wave. The OCT image looks somewhat like the bottom topography cross sections we used to get during our acoustical surveys of eelgrass on the seafloor.

As it turned out, OCT was the exact tool necessary to confirm the diagnosis of my eye problem, and that explains why I had to go to Comox for it – I imagine that these machines are relatively few and far between. So, I do have an epiretinal membrane in my right eye, and something called a “macular pseudohole” (see image below) which looks like a macular hole, but isn’t.
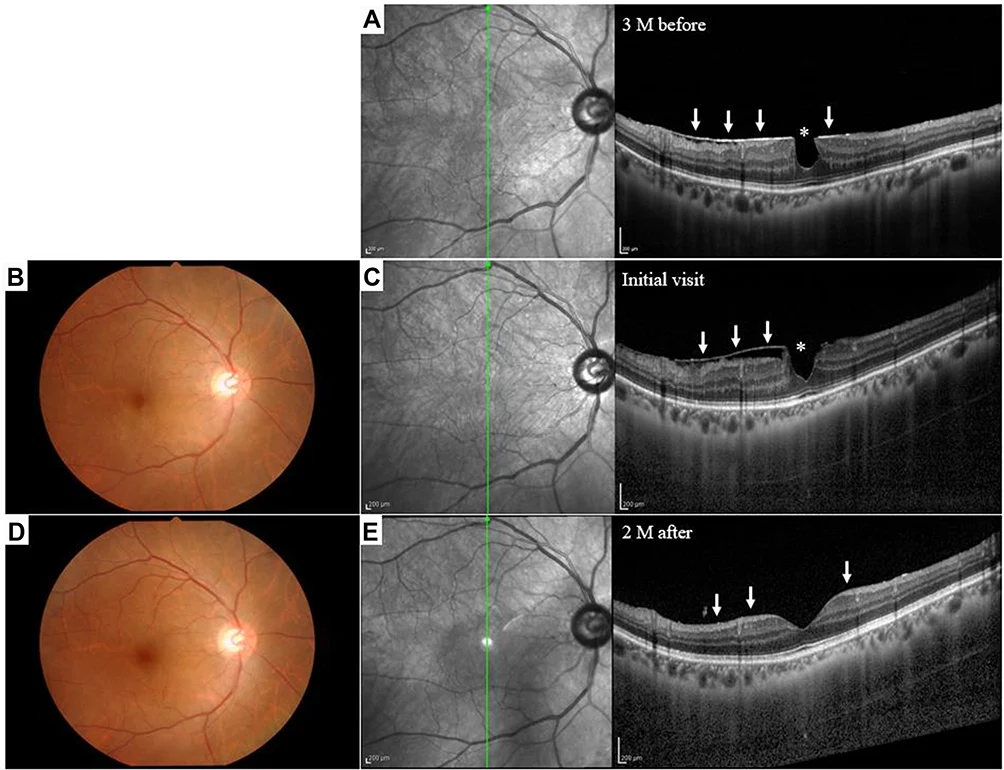
Shown below is an example of the diagnosis of an epiretinal membrane using OCT (not from my eyes).

An epiretinal membrane can either (1) go away by itself; (2) stay the same; or (3) get worse and require a surgical removal (which can be done at either Victoria or Vancouver). The surgical procedure has a bit of risk and, as a result, the recommendation is to hold out as long as possible. So, for the moment, I will have to go to Comox every six months for an OCT scan to determine if there have been any changes.
I also have an “Amsler grid”, a card gridded with vertical and horizontal lines which I can use to see if the situation is changing by observing the distortions in the lines.


I’m very glad that I don’t have macular degeneration or cancer (one of my aunts is losing an eye from skin cancer, another lost her vision from macular degeneration). The only real downside so far is that the ophthalmologist uses a really strong atropine sulfate solution for pupil dilation. I’ve had the drops before, and they usually only affect me for a couple of hours, but this time the effect took over six hours to wear off. Part way through that, I drove back to Sayward, which turned out not to be such a good idea (the truck and the three of us survived, but there were a few iffy moments). I won’t be doing that again, so it’ll be a hotel/motel room or camping out when I go again in May for my next check up.